Parts of an instrument
 |
| Copyright 2013 Wolfers Kluwer Health | Lippincott Williams & Wilkins |
All Dental hand instruments, be it a dental mirror, probe, scalers or curets are composed of
A. Handle
B. Shank
C. Working-End
Handle
The handle is where one would hold or grasp the instrument and there is usually a serrated to aid in gripping to optimise control of the instrument and reduce fatigue when working in the oral environment.
Shank
The Shank connects the handle to the working end and allows for adaptation of the working end to the tooth surface. It is also used to differentiate between instruments used for posterior (complex) and anterior (simple) teeth.
 |
| The shank is composed of the functional shank and lower or terminal shank. |
Functional shank : extends from working end to the bend before the handle
Terminal shank: extends from the working end to the first bend

Working End
The working end is what is in contact with the tooth surface and/or the portion of the instrument that does the work as it's name suggest.
The working end has a number of surface depending on the instrument. Most periodontal hand instruments such as sickle scalers and curettes have :

Sickle scalers will always have a tip which is sharp _ Curettes have toes which are rounded.
When using these instruments, we work with the first 1-2mm of the instrument.
Another way to differentiate between sickle scalers and curettes is by theircross section.
(If you require graphic aid, it's always wise to determine whether it is shaped like a toblerone chocolate or a kinder bueno)
 If it's a toblerone -Sickle scaler
If it's a toblerone -Sickle scaler
 If it's like an inverted kinder bueno- Curette.
If it's like an inverted kinder bueno- Curette.
My point is that although both instruments have similar structure and looks, they can serve different purpose.
Shanks can come in a variety of length.
-Short
-Standard (A)
-Extended (B)
Shanks can also be simple (straight) or complex (bent). 
As a rule of thumb: Simple - Anterior teeth application
(left)
Complex - Posterior teeth application
(right)Working End
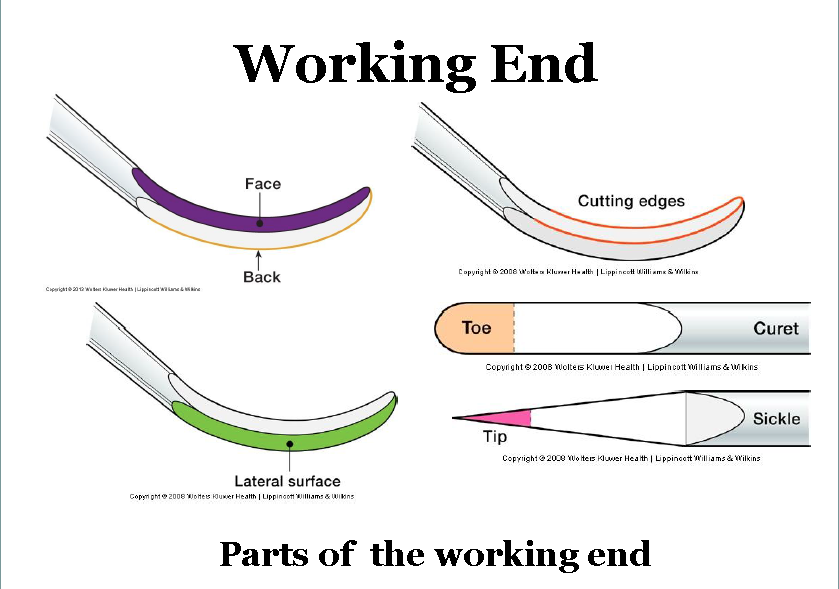
The working end is what is in contact with the tooth surface and/or the portion of the instrument that does the work as it's name suggest.
The working end has a number of surface depending on the instrument. Most periodontal hand instruments such as sickle scalers and curettes have :
- Face
- Back
- Lateral Surface
- Cutting edges
- Tip or Toe
And the working end can be segmented into 3 parts
1) Toe/Tip
2) Middle
3) Heel

You see, the working tip/toe is used for kicking and you want this part to land on that chav's...
The picture below shows the parts of the working ends of these specialised instruments.
1) Toe/Tip
2) Middle
3) Heel
 |
| Courtesy of my lecturer, Dr C.Gonzales-Marin |
The picture below shows the parts of the working ends of these specialised instruments.
Here's another diagram because we <3 Diagrams!
Sickle scalers will always have a tip which is sharp _ Curettes have toes which are rounded.
When using these instruments, we work with the first 1-2mm of the instrument.
Another way to differentiate between sickle scalers and curettes is by their
- Face the tip/toe of the instrument towards yourself
- Determine if the cross section is triangular or semi-circular
(If you require graphic aid, it's always wise to determine whether it is shaped like a toblerone chocolate or a kinder bueno)
TobleronesSickle scalers are for Supra-gingival scaling ONLYKinder BuenosCurettes are for BOTH Supra and Sub-gingival scaling.
My point is that although both instruments have similar structure and looks, they can serve different purpose.
























